Resources Topic 2: Causes, epidemiology, socio-cultural determinants
This graphic provides a nice summary of the relationship between socioeconomic, behavioural and biologic risk factors for CVD.
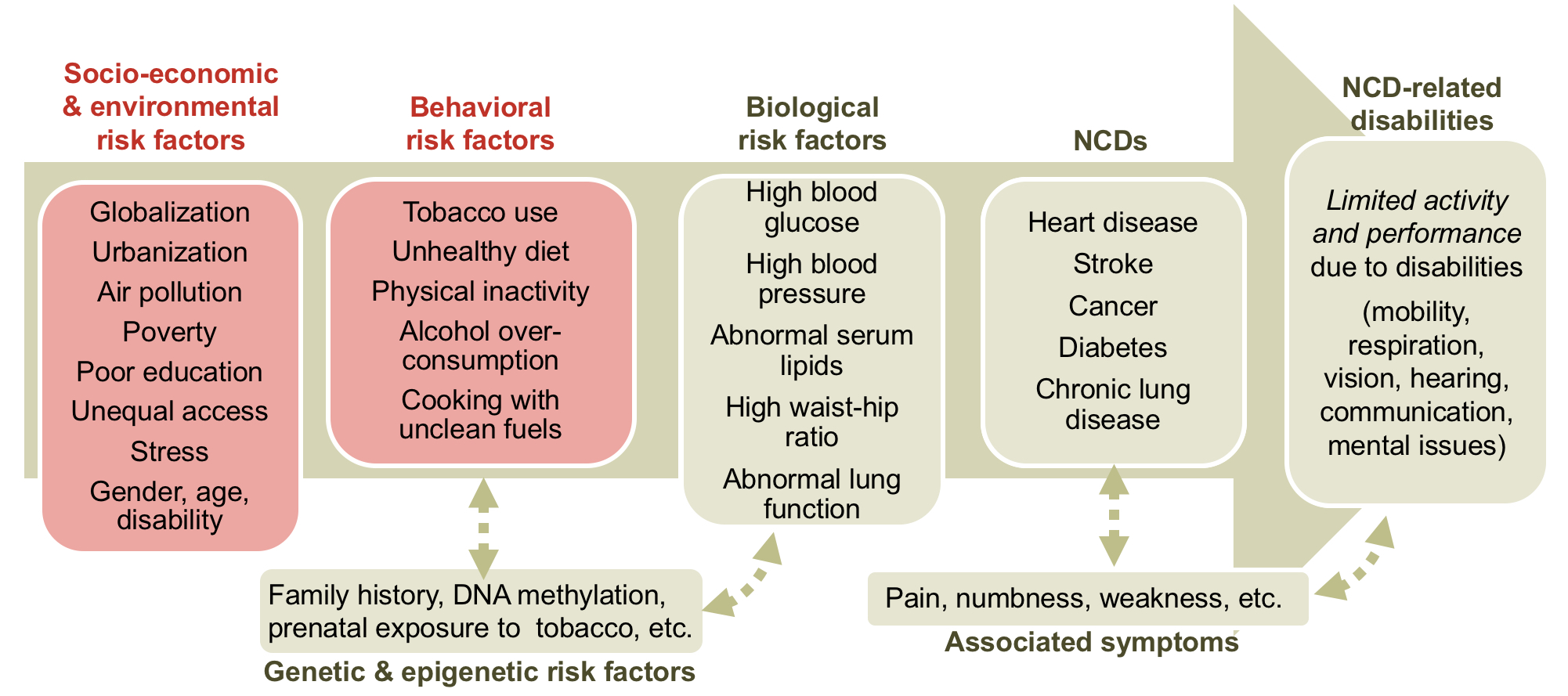
Determinants and chronic conditions of NCDs (modified from Dans et al., 2011 by Medicus Mundi Switzerand) from Health Promotion and Health Literacy: Toward transformative action for non-communicable diseases.
We know a considerable amount about the causes of CVD, with evidence going back many decades, but there is emerging evidence and considerable debate still. While the graphic above is a nice summary, here are some issues to which we should pay attention.
Risk factors in a global setting. This paper Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study, published in 2004 its summary found: "Abnormal lipids, smoking, hypertension, diabetes, abdominal obesity, psychosocial factors, consumption of fruits, vegetables, and alcohol, and regular physical activity account for most of the risk of myocardial infarction worldwide in both sexes and at all ages in all regions." (Note: fruit, vegetable and alcohol consumption and regular physical activity were associated with a reduced risk, the others with an increased risk).
The same team provides a more recent update in Cardiovascular Risk and Events in 17 Low-, Middle-, and High-Income Countries. Using a validated score for quantifying risk-factor burden without the use of laboratory testing, they found "Although the risk-factor burden was lowest in low-income countries, the rates of major cardiovascular disease and death were substantially higher in low-income countries than in high-income countries. The high burden of risk factors in high-income countries may have been mitigated by better control of risk factors and more frequent use of proven pharmacologic therapies and revascularization"
A landmark study is summarised: "the WHO MONICA (Monitoring trends and determinants in cardiovascular disease) project was organized as a monitoring system to assess trends and determinants of cardiovascular mortality, incidence and case fatality from the mid 1980 s to the mid 1990 s in 38 populations in 21 countries worldwide. Altogether some 13 million people were monitored over a 10 year period. 166,000 myocardial infarction patients were registered and more than 300,000 men and women were sampled and examined for their cardiovascular risk factors and many other health data. In Western countries, where the CHD mortality decline was on average 2-3 % annually, two thirds of this decline could be explained by a decline in CHD incidence and one third by a decline in CHD case fatality. When relating risk factor changes to changes in CHD event rates in men over a time period of 10 years in all MONICA populations it turned out that the greatest contribution to the CHD decline came from a decrease in smoking. On a worldwide scale the Seven Countries Study, the Framingham Heart Study and the WHO MONICA Project have contributed most to the development of epidemiology and prevention of cardiovascular diseases."
A paper The contributions of risk factor trends and medical care to cardiovascular mortality trends found: "Ischaemic heart disease, stroke, and other cardiovascular diseases (CVDs) are responsible for an estimated 17.5 million annual deaths in the world. If account is taken of population aging, death rates from CVDs are estimated to be steadily decreasing in the world as a whole, and in regions with reliable trend data. The declines in high-income countries and some countries in Latin America have been ongoing for decades with no indication of slowing. In high-income countries, these positive trends have broadly coincided with, and benefited from, declines in smoking and physiological risk factors like blood pressure and serum cholesterol. Improvements in medical care, including effective primary prevention through management of physiological risk factors, better diagnosis and treatment of acute CVDs, and post-hospital care of those with prior CVDs, are also likely to have contributed to declining CVD event and death rates, especially in the past 40 years.".
The paper Cardiovascular disease and hypertension in sub-Saharan Africa: burden, risk and interventions points the finger at high blood pressure as the major risk factor, and summarises: "Cardiovascular disease, including stroke, heart failure and kidney disease, has been common in sub-Saharan Africa for many years, and rapid urbanization is causing an upsurge of ischaemic heart disease and metabolic disorders. At least two-thirds of cardiovascular deaths now occur in low- and middle-income countries, bringing a double burden of disease to poor and developing world economies. High blood pressure (or hypertension) is by far the commonest underlying risk factor for cardiovascular disease. Its prevention, detection, treatment and control in sub-Saharan Africa are haphazard and suboptimal. This is due to a combination of lack of resources and health-care systems, non-existent effective preventive strategies at a population level, lack of sustainable drug therapy, and barriers to complete compliance with prescribed medications. The economic impact for loss of productive years of life and the need to divert scarce resources to tertiary care are substantial."
Poverty. The paper Poverty and risk factors for non-communicable diseases in developing countries: a systematic review finds: "in high-income countries, low socioeconomic status is associated with use of tobacco and alcohol, physical inactivity, and poor diet...After review of 4242 records, 75 studies met our inclusion criteria, representing 2 135 314 individuals aged more than 10 years from 39 LLMICs. Most studies found that, compared with high socioeconomic groups, lower status groups had a high prevalence of tobacco and alcohol use (odds ratios up to 18·8 and 3·5, respectively). Most studies also found that lower socioeconomic groups consumed less fruit, vegetables, fish, and fibre (odds ratios negligible to 12·9, depending on context). Higher socioeconomic groups were up to 4·4 times less physically active...there is clear evidence that the burden of behavioural risk factors is affected by socioeconomic position within LLMICs. Governments seeking to meet Sustainable Development Goal 3.4—reducing premature mortality from non-communicable diseases by a third by 2030—should leverage their development budgets to address the poverty–health nexus in these settings."
Diabetes. Let's not forget diabetes and an excellent review from a Lancet Commission Diabetes in sub-Saharan Africa: from clinical care to health policy suggests: "Diabetes is an exemplar risk factor of cardiovascular disease in that its prevalence tracks the transitions that lead to the precursors of cardiovascular disease—namely obesity and overweight. The prevalence of diabetes is increasing rapidly in sub-Saharan Africa. If left untreated, diabetes leads to a plethora of complications, both microvascular and macrovascular, that affect multiple physiological systems. Additionally, diabetes is closely associated with other cardiovascular risk factors, including hypertension and hypercholesterolaemia, which interact to exacerbate the risk of adverse outcomes. Thus, diabetes requires an interconnected, broad-based health system for its effective management. Improving the processes of care for people with diabetes should lead to improvement of health systems for many other conditions."
The paper Diabetes and ethnic minorities suggests that ethnicity is an important risk factor for developing both type 2 diabetes and heart disease. Globally, type 2 diabetes prevalence ranges from less than 2% in China to 50% among Mexican Pima Indians. In the UK, type 2 diabetes is 3-5 times more prevalent in African-Caribbean and South Asian groups respectively compared to the white European population. In the US, half of all black adults have some form of cardiovascular disease compared to only one in three white adults (Race and ethnicity: Clues to your heart disease risk?).
Nutritional transition. Changes in dietary habits may exacerbate non-communicable disease risk in individuals with a genetic predisposition. An example of this is shown in South Asian individuals who have migrated to Europe (Changes in dietary habits after migration and consequences for health: a focus on South Asians in Europe). The typical diet change for these individuals shows increased energy and fat intake along with a transition from high fibre foods to more refined alternatives, post-migration. It is likely that this nutritional transition may have contributed to a higher risk of obesity, type 2 diabetes and CVD.
Fat or sugar? Fat, Sugar, Whole Grains and Heart Disease: 50 Years of Confusion has summarised as folows: "During the 1970s some investigators proposed that refined carbohydrates, especially sugar and a low intake of dietary fiber, were major factors in coronary heart disease (CHD). This suggestion was eclipsed by the belief that an excess intake of saturated fatty acids (SFA) was the key dietary factor, a view that prevailed from roughly 1974 to 2014. Findings that have accumulated since 1990 inform us that the role of SFA in the causation of CHD has been much exaggerated. A switch from SFA to refined carbohydrates does not lower the ratio of total cholesterol to HDL-cholesterol in the blood and therefore does not prevent CHD. A reduced intake of SFA combined with an increased intake of polyunsaturated fatty acids lowers the ratio of total cholesterol to HDL-cholesterol; this may reduce the risk of CHD. The evidence linking carbohydrate-rich foods with CHD has been steadily strengthening. Refined carbohydrates, especially sugar-sweetened beverages, increase the risk of CHD. Conversely, whole grains and cereal fiber are protective. An extra one or 2 servings per day of these foods increases or decreases risk by approximately 10% to 20%."
The fat vs carbohydrate debate was further complicated by the findings of The Prospective Urban Rural Epidemiology (PURE) study, a large, epidemiological cohort study of adults aged 35-70 years from 18 countries, published in 2017. It concluded that a “high carbohydrate intake was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality." However there have been questions about the methodology and conclusions PURE study makes headlines, but the conclusions are misleading. This demonstrates the complexity of analysing the relationship between nutritional factors and non-communicable diseases
Air Pollution: An Emerging Risk Factor. As well as socioeconomic and behavioural risk factors, an individual’s environment plays a key role in the development of cardiovascular disease. Air pollution can be seen as an emerging risk factor due to the rapid urbanisation of lower income countries and the increasing global impact of climate change. Air Pollution and Cardiovascular Disease outlines in more detail the role that air pollution has on cardiovascular disease.
So we see that despite the many years of research into CVD, there are still many questions. These include the best way to prevent and reduce the burden of disease in populations - as we explore in later sections of the course.