Resources Topic 3
Distinguish between primary and secondary prevention programmes and between population-based and individual-based interventions.
Geoffrey Rose identified the differences between population and individual based intervention. Strategies can either target those at high risk of developing disease, or can work on the whole population to prevent the causes of the disease. His original paper 'Sick Individuals and Sick Populations' is reprinted here.
An excellent paper, Will Cardiovascular Disease Prevention Widen Health Inequalities, describes the high risk and population approaches, and discusses their potential impacts. Their summary points are listed below:
- The primary prevention of cardiovascular disease (CVD) is dependent on the effective reduction of the major risk factors for CVD, particularly tobacco control and a healthier diet.
- The high-risk approach to prevent CVD typically involves population screening. Those exceeding a risk threshold are then given lifestyle advice and/or tablets to reduce blood cholesterol and blood pressure.
- Evidence suggests this high-risk approach typically widens socioeconomic inequalities. Such inequalities have been reported in screening, healthy diet advice, smoking cessation, statin and anti-hypertensive prescribing, and adherence.
- The alternative approach is population-wide CVD prevention. For example, legislating for smoke-free public spaces, banning dietary transfats, or halving daily dietary salt intake. Such strategies are generally effective and cost-saving; there is also increasing evidence that they can reduce health inequalities.
- We conclude that screening and treating high-risk individuals represents a relatively ineffective CVD prevention approach that typically widens social inequalities.
Identify international initiatives to change health policies to reduce the burden of CVD and Diabetes
Here are some WHO web sites which identify their programmes:
Strategic priorities of the WHO Cardiovascular Disease programme. In summrary: The WHO Programme on Cardiovascular Diseases works on prevention, management and monitoring of cardiovascular disease (CVD) globally. It aims to develop global strategies to reduce the incidence, morbidity and mortality of cardiovascular diseases (CVD) by:
- effectively reducing CVD risk factors and their determinants;
- developing cost effective and equitable health care innovations for management of CVD;
- monitoring trends of CVD and their risk factors.
Regional activities to the global CVD strategy. You can see what is happening in your region.
Diabetes Action now. WHO also has an active programme for diabetes.
Identify the evidence base that has led to the development of interventions, and which of these initiatives have led to improvements in health outcomes
Scaling up interventions for chronic disease prevention: the evidence is an excellent review of the evidence - although dated now, the key points from the paper are still relevant - see below:
- "Interventions to reduce chronic diseases should be both cost effective and financially feasible before scaling up in countries of low or middle income
- Tobacco control, salt reduction, and a multidrug strategy to treat individuals with high-risk cardiovascular disease are three interventions that have strong cost effectiveness data for scale-up in such countries
- Further studies to assess the best national policies to reduce consumption of saturated and trans fats at a reasonable cost are needed before scaling up such interventions
- Several other interventions do not have sufficient cost effectiveness data for countries of low or middle income, but their effectiveness data are so compelling that their implementation, along with critical assessment, should be implemented in such settings
- There are limited data for structural interventions directed at the social determinants of chronic diseases, including health systems. This is an area that deserves immediate focused attention"
As stated in Diabetes in sub-Saharan Africa: from clinical care to health policy, "When health resources are severely limited, difficult choices must often be made in the face of competing priorities. Our review of the challenges involved makes it clear that models of diabetes care for use in high-income countries are neither appropriate nor affordable in low-income or middle-income countries. We advocate the pursuit of a utilitarian approach to the provision of diabetes care in most sub-Saharan African settings, involving widely available inexpensive treatments for prevention of complications alongside strong public health measures to prevent increases in the prevalence of obesity and diabetes". This extensive report also identifies the gaps in evidence that still exist.
Disease Control Priorities in Developing Countries contains the key resource for this Topic with its review of the evidence for interventions Please look particularly at the chapters on cardiovascular and related diseases - you will find the overview chapter here http://dcp-3.org/chapter/2306/overview and when you click on the sections on the lefthand column you can see each of the chapters. The summary is:
"Adults living in low- and middle-income countries (LMICs) face high risk for death, disability, and impoverishment from cardiovascular, respiratory, and related disorders (CVRDs). Most of these disorders prove preventable or, if they occur, remain medically treatable to improve longevity and reduce disability. Optimal prevention and treatment—which require resources but also consistent and persistent therapeutic compliance—remain a challenge even in high-income countries (HICs). Additionally, in LMICs, the limited capacity to detect these silent diseases and provide early treatment contributes to the rapid emergence of advanced complications and premature death. Effective prevention strategies remain underutilized, and primary care centers require strengthening to treat the current and growing burden of CVRDs. Cost-effective prevention policies and treatments for CVRDs remain possible to implement in LMICs, and universal health care that includes care for CVRDs provides benefits beyond individual health to financial protection of families. Many important issues remain uncertain, however, especially given the scarcity of LMIC economic evidence, including research in areas likely to produce high public benefit and new technologies, medications, and delivery platforms."
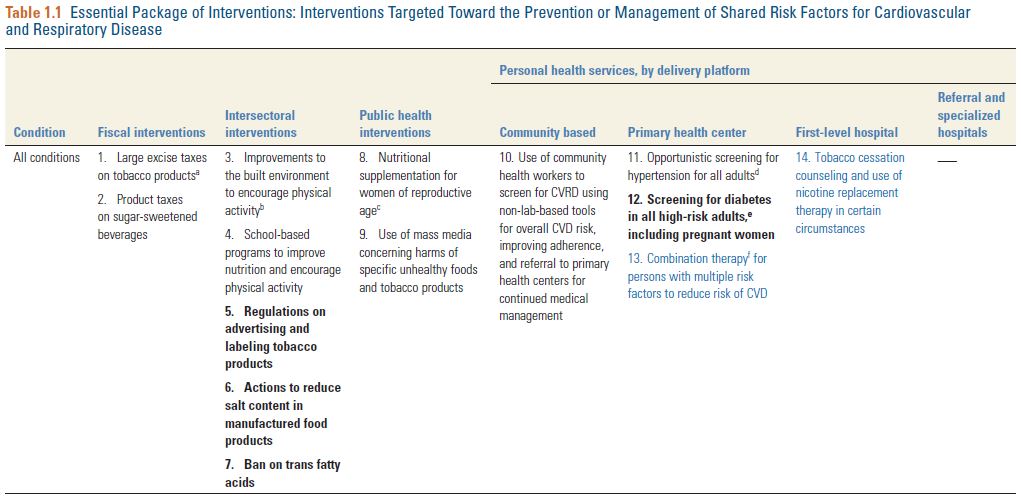
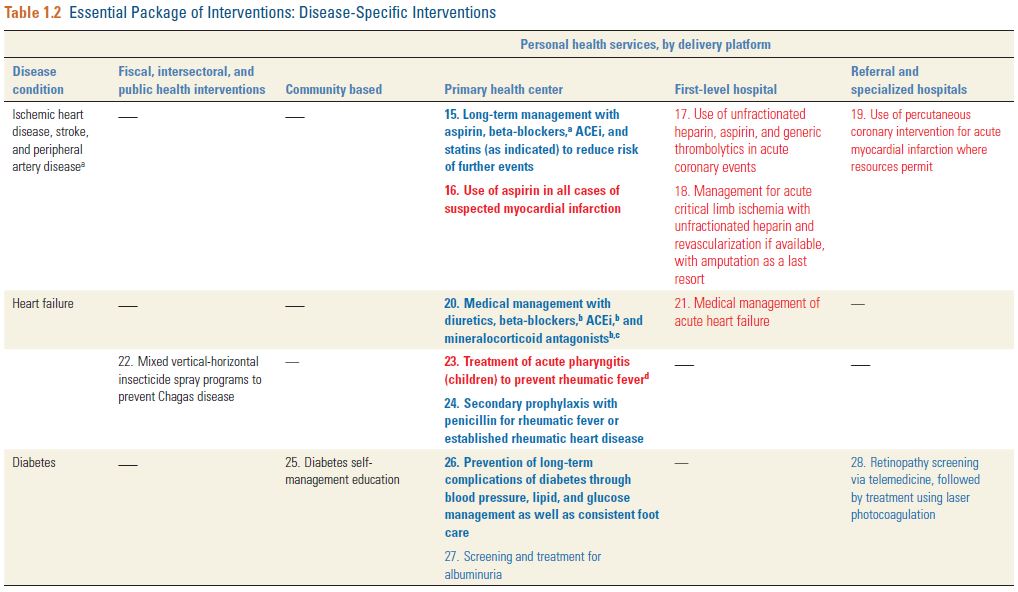
You can download the DCP3 chapter Cardiovascular, Respiratory, and Related Disorders: Key Messages and Essential
Interventions to Address Their Burden in Low- and Middle-Income Countries where you will see that it identifies an 'essential package of interventions', and these are summarised in the two tables from the chapter, copied below: