Obesity and health
Definition
From the World Health Organization (WHO) website Obesity “Overweight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health. A crude population measure of obesity is the body mass index (BMI), a person’s weight (in kilograms) divided by the square of his or her height (in metres). A person with a BMI of 30 or more is generally considered obese. A person with a BMI equal to or more than 25 is considered overweight.”
However, this might differ in different populations such as in Asian populations who develop type 2 diabetes and metabolic risk at a younger age and lower BMI than Western populations, hence the WHO has proposed lower BMI action points of 23 and 28 for Asian adults. Obesity Prevention
Obesity Definition makes the point that the above definition may not apply to children and adolescents (see also Obesity and overweight). There are other measures which have been used in epidemiological studies – abdominal obesity measured by waist size or wait to hip ratio. More complex measures of body fat using specialised equipment are also available.
Measurement
BMI-related errors in the measurement of obesity comments: "Body mass index (BMI) has various deficiencies as a measure of obesity, especially when the BMI measure is based on self-reported height and weight. BMI is an indirect measure of body fat compared with more direct approaches such as bioelectrical impedance. Moreover, BMI does not necessarily reflect the changes that occur with age. The proportion of body fat increases with age, whereas muscle mass decreases, but corresponding changes in height, weight and BMI may not reflect changes in body fat and muscle mass."
Measurement of overweight and obesity an urban slum setting in sub-Saharan Africa: a comparison of four anthropometric indices finds: "There exists a moderate level of correlation and a remarkable level of discordance among the four anthropometric indices (Body Mass Index, Waist Circumference, Waist to Hip Ratio, and Waist to Height Ratio) with regard to the ascertainment of abnormal body composition in an urban slum setting in Africa. Waist circumference better predicted hypertension and hyperglycemia while waist to height ratio better predicted hypercholesterolemia."
What about self report? Examining validity of body mass index calculated using height and weight data from the US driver license "Individuals, on average, tend to overestimate their height and underestimate their weight. Consequently, the value of BMI calculated using driver license records is lower than BMI calculated using clinical measurements. The discrepancy varies by age and by BMI category. Despite the discrepancy, BMI based on self-reported height and weight allows for accurate categorization of individuals at the higher end of the BMI scale, such as the obese. When used as predictors of relative risk of type II diabetes, both sets of BMI values yield similar risk estimates."
BMI is a good measure of health after all, new study finds is the reported conclusion of the lead author of a detailed study: "...simple BMI gives very similar answers to more detailed measures. This is good news since BMI is widely measured and costs virtually nothing."
Please see this more detailed description of the different measures of body composition and their implications for health outcomes.
Extent of the problem
Obesity and overweight Key facts from WHO
- Worldwide obesity has nearly tripled since 1975.
- In 2016, more than 1.9 billion adults, 18 years and older, were overweight. Of these over 650 million were obese.
- 39% of adults aged 18 years and over were overweight in 2016, and 13% were obese.
- Most of the world's population live in countries where overweight and obesity kills more people than underweight.
- 40 million children under the age of 5 were overweight or obese in 2018.
- Over 340 million children and adolescents aged 5-19 were overweight or obese in 2016.
- Obesity is preventable.
The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action reports: "Over the past four decades, obesity in children of all ages has increased worldwide, as it has for adults. However, obesity appears to have increased more rapidly in 5–19 year olds than in younger children, with an eight-fold increase between 1975 and 2016. This contrasts with an approximate doubling in obesity rates in children aged 2–4 years between 1980 and 2015, albeit using metrics that are not directly comparable. There is heterogeneity in the levels and trends in obesity prevalence between regions and countries, depending on the stage of the global obesity epidemic they are experiencing. In particular, there has been some flattening of trends, especially among those with high socioeconomic status in high-income countries."
Health Effects of Overweight and Obesity in 195 Countries over 25 Years finds: "In 2015, a total of 107.7 million children and 603.7 million adults were obese. Since 1980, the prevalence of obesity has doubled in more than 70 countries and has continuously increased in most other countries. Although the prevalence of obesity among children has been lower than that among adults, the rate of increase in childhood obesity in many countries has been greater than the rate of increase in adult obesity."
Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults includes the following trends in obesity by age (shown here for men)
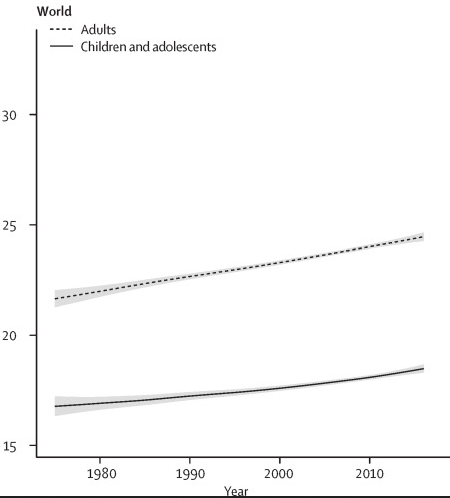
and also finds: "The rising trends in children's and adolescents' BMI have plateaued in many high-income countries, albeit at high levels, but have accelerated in parts of Asia, with trends no longer correlated with those of adults."
Back to measurement, however! Determining the worldwide prevalence of obesity comments that: "Systematic reviews of a large amount of high-quality and consistent evidence show that the use of BMI to define obesity (the degree of excess body fat) is highly specific, but has low to moderate sensitivity. As a result, BMI-based estimates of obesity prevalence are highly conservative for all ages and both sexes. Around half of all adults with excess body fat are defined as non-obese according to BMI, and at least 25–50% of children and adolescents defined as having a healthy BMI-for-age will also have excess body fat. These systematic reviews are based largely on evidence from European and western populations. In many other populations, the bias associated with the use of BMI is worse, leading to more pronounced underestimates of obesity prevalence, and complicating global comparisons."
Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges shows: "Obesity is rising in every region of the world, and no country has been successful at reversing the epidemic once it has begun. In low- and middle-income countries (LMICs), overweight is higher in women compared with men, in urban compared with rural settings, and in older compared with younger individuals; however, the urban–rural overweight differential is shrinking in many countries. Overweight occurs alongside persistent burdens of underweight in LMICs, especially in young women."
Socioeconomic status
Obesity Prevention finds that: "Within countries, obesity is related to socioeconomic status. In many LMICs, body weight is positively associated with socioeconomic status, which contrasts with general patterns observed in the United States and other HICs, where body weight tends to be inversely associated with socioeconomic status. The association between socioeconomic status and body weight is thought to depend on the level of economic development in the country."
Economic costs
Economic Costs reports that the costs are high, and include:
"Direct costs are those that result from outpatient and inpatient health services (including surgery), laboratory and radiological tests, and drug therapy.
Indirect costs, which have been defined as “resources forgone as a result of a health condition,” fall into various categories:
- Value of lost work. Days missed from work are a cost to both employees (in lost wages) and employers (in work not completed). Obese employees miss more days from work due to short-term absences, long-term disability, and premature death than nonobese employees. They may also work at less than full capacity (also known as presenteeism).
- Insurance. Employers pay higher life insurance premiums and pay out more for workers’ compensation for employees who are obese than for employees who are not.
- Wages. Some studies have shown that obesity is associated with lower wages and lower household income."
The costs of overweight adds that: "Many health economists are now focusing on the broad societal costs of being overweight, including early retirement, efficiency at work, and prospects of promotion. These societal costs are now estimated to account for 60% of the total costs of being overweight or obese...In 2014, the McKinsey Institute estimated the economic burden of being overweight or obese at US$2 trillion, matching that of smoking and all armed conflict."
Causes of obesity
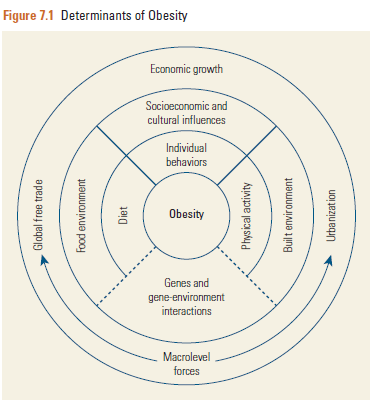
The picture from Disease Prevention Control Project 3 (DCP3) shows the multiple ‘causes’ or determinants of obesity. Some are at the individual and some at the societal level.
The paper Upstream Determinants of Adult Obesity describes the predisposing factors for obesity as: "Over-consumption of high-energy foods and a lack of physical activity are the main behavioural risk factors for people to develop obesity. These behaviours are influenced by a range of individual-level factors which are nested within contexts that contain influencing characteristics further upstream.
In the process of domestication, we went from hunting and gathering food to planting and planning food production. We have advanced our methods to secure food resources and have created environments that make access to foods easier. Simultaneously, smart engineering obviated heavy manual work such that populations sit more and move less, despite busier schedules. In other words, we have adapted the context we live in. Up until a few decades ago, our energy intake and energy expenditure remained in balance, but in many developed countries we have reached a tipping point whereby excess energy has resulted in increased rates of obesity. The relative price of calorie-dense foods and beverages has decreased in tandem with the observed rapid increase in consumption of energy-dense products while physical activity can now be avoided almost everywhere and anytime, which has led to a decrease in our energy expenditure.
Upstream determinants of public health are usually defined as those overarching factors that are largely beyond the control of the individual and which have significant spill-over effects on other more proximal - or downstream - determinants of health."
Globalisation is clearly an ‘upstream’ determinant, but its role in the development of obesity is controversial.
The impact of economic, political and social globalization on overweight and obesity in the 56 low and middle income countries finds: "Anecdotal and descriptive evidence has led to the claim that globalization plays a major role in inducing overweight and obesity in developing countries, but robust quantitative evidence is scarce. We undertook extensive econometric analyses of several datasets, using a series of new proxies for different dimensions of globalization potentially affecting overweight in up to 887,000 women aged 15–49 living in 56 countries between 1991 and 2009. After controlling for relevant individual and country level factors, globalization as a whole is substantially and significantly associated with an increase in the individual propensity to be overweight among women. Surprisingly, political and social globalization dominate the influence of the economic dimension. Hence, more consideration needs to be given to the forms of governance required to shape a more health-oriented globalization process."
Although:
What is driving global obesity trends? Globalization or “modernization”? suggests that: "Global increases in overweight/obesity appear to be driven more by domestic processes including economic development, urbanization and women’s empowerment, and are less clearly negatively impacted by external globalization processes suggesting that the harms to health from global trade regimes may be overstated."
Among adolescents, this paper reviews the evidence: Behavioral, contextual and biological factors associated with obesity during adolescence: A systematic review "40 studies published between the year 2000 and 2018 were included. A positive consistent association between genetic factors and obesity during adolescence was found. Also, there is evidence to support the association between socioeconomic status and obesity. There was conflicting evidence for the contribution of dietary intake, physical activity, sedentary behavior, sleep, food store environment, school food environment. For the remaining factors no associations were found, or no conclusions could be drawn due to the limited number of studies identified."
The journalist’s view - its the composition of the diet (blame big business)
We’re in a new age of obesity. How did it happen? You’d be surprised (by George Monbiot) "Yes, we ate more in 1976, but differently. Today, we buy half as much fresh milk per person, but five times more yoghurt, three times more ice cream and – wait for it – 39 times as many dairy desserts. We buy half as many eggs as in 1976, but a third more breakfast cereals and twice the cereal snacks; half the total potatoes, but three times the crisps. While our direct purchases of sugar have sharply declined, the sugar we consume in drinks and confectionery is likely to have rocketed (there are purchase numbers only from 1992, at which point they were rising rapidly….In other words, the opportunities to load our food with sugar have boomed. As some experts have long proposed, this seems to be the issue.
The shift has not happened by accident. As Jacques Peretti argued in his film The Men Who Made Us Fat, food companies have invested heavily in designing products that use sugar to bypass our natural appetite control mechanisms, and in packaging and promoting these products to break down what remains of our defences, including through the use of subliminal scents. They employ an army of food scientists and psychologists to trick us into eating more than we need... Just as jobless people are blamed for structural unemployment, and indebted people are blamed for impossible housing costs, fat people are blamed for a societal problem. But yes, willpower needs to be exercised – by governments. Yes, we need personal responsibility – on the part of policymakers. And yes, control needs to be exerted – over those who have discovered our weaknesses and ruthlessly exploit them."
But what about genetics?
A nice summary comes from Genes Are Not Destiny: "Having a better understanding of the genetic contributions to obesity-especially common obesity-and gene-environment interactions will generate a better understanding of the causal pathways that lead to obesity. Such information could someday yield promising strategies for obesity prevention and treatment. But it’s important to remember that overall, the contribution of genes to obesity risk is small, while the contribution of our toxic food and activity environment is huge. As one scientist wrote, “Genes may co-determine who becomes obese, but our environment determines how many become obese.” That’s why obesity prevention efforts must focus on changing our environment to make healthy choices easier choices, for all."
Health effects of obesity
Health Effects of Overweight and Obesity in 195 Countries over 25 Years summarises: "High BMI accounted for 4.0 million deaths globally, nearly 40% of which occurred in persons who were not obese. More than two thirds of deaths related to high BMI were due to cardiovascular disease. The disease burden related to high BMI has increased since 1990; however, the rate of this increase has been attenuated owing to decreases in underlying rates of death from cardiovascular disease."
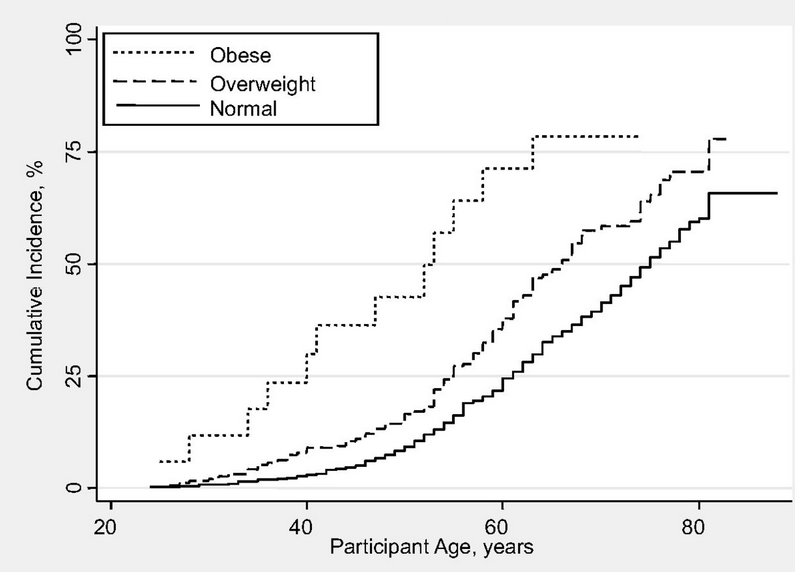
This may at least partly mediated through the relationship between obesity and hypertension, as in Body Mass Index and Risk of Incident Hypertension Over the Life Course "After adjustment for time-dependent number of cigarettes smoked, cups of coffee taken, alcohol intake, physical activity, parental premature hypertension, and baseline BMI, the rate of change in BMI over the life course increased the risk of incident hypertension in a dose-response fashion, with the highest risk among men with the greatest increase in BMI" The picture from this paper shows the incidence over time of hypertension in those according to their BMI
Margaret Chan, previously Director General of WHO says in Obesity and diabetes: the slow-motion disaster Keynote address at the 47th meeting of the National Academy of Medicine "Obesity contributes to the risk for cardiovascular diseases and some cancers. But the role of adiposity as an independent risk factor is strongest for diabetes. Moreover, diabetes with its costly complications, including blindness, limb amputations, and the need for dialysis, can place an extraordinary long-term burden on health budgets and household finances."
Although most attention is paid to cardiovascular disease and diabetes, there is also a risk for a number of cancers as desribed here: Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults "The heaviest members of this cohort (those with a body-mass index [the weight in kilograms divided by the square of the height in meters] of at least 40) had death rates from all cancers combined that were 52 percent higher (for men) and 62 percent higher (for women) than the rates in men and women of normal weight. … Increased body weight was associated with increased death rates for all cancers combined and for cancers at multiple specific sites."